

There seems to be a huge misunderstanding around the etiology of type 2 diabetes and how we can successfully cure rather than manage it.
This blog post comes in on the tails of my conversation with Tim Noakes via Twitter, and him blocking me after I challenged his viewpoint that the only way to treat diabetes is with a low-carbohydrate ketogenic diet.
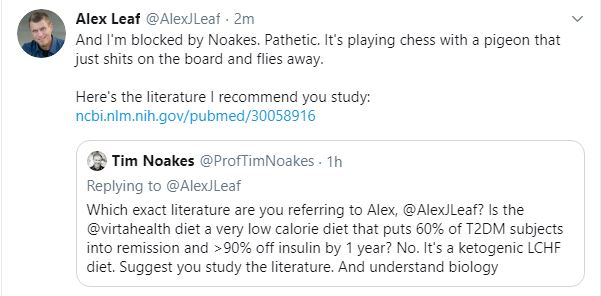
Let’s look at this Virta Health study that Noakes references as evidence that treating type 2 diabetes requires a ketogenic diet. Over the course of 2 years, participants followed either a ketogenic diet or usual care.1
With 57% of the participants using medications at baseline, only 27% were using after 2 years. Those taking exogenous insulin reduced their average dose by 81%, and the number of insulin users was reduced from 30% to 11%. Despite lower medication usage, there were significant reductions in HbA1c, fasting glucose, and fasting insulin.
Ultimately, 53% of the participants were said to have “reversed” their diabetes (HbA1c < 6.5% without medications except metformin), 11% were said to be in “partial remission” (HbA1c of 5.7–6.5% without any medication), and 7% were said to be in “complete remission” (HbA1c of <5.7% without any medication).
But guess what? They also lost a shit-ton of weight. Half the participants lost more than 10% of their body weight. So, are the benefits owed to a ketogenic diet or to fat loss? Probably both, most notably the fat loss.


Ignoring that Noakes can’t even properly cite the details of the study he thinks I need to study, none of these findings are surprising.
Obviously, reducing the amount of carbohydrates you eat will lower markers of glycemia since dietary carbohydrate are the primary driver of glycemic changes.
But this is artificial, and that was my point in the discussion with Noakes. If you take someone with Celiac disease and remove the gluten from the diet, then is their disease gone or simply being managed by the dietary changes?
In order to cure Celiac disease, you can’t just remove the insulting component of the diet, you have to address the disease processes, which in this case would be preventing the autoimmune attack against the intestinal cells when gluten is consumed.
Eating a ketogenic diet is just symptom management for diabetes unless you simultaneously address the cause of the diabetes (which is not eating carbohydrates).
The cause of diabetes
The cause of type-2 diabetes is almost always an issue with surpassing one’s personal fat threshold.2 I discuss this idea in a previous article of mine: Is healthy obesity a thing?
Basically, we all have an amount of fat we can store safely (due to genetic, environmental, and lifestyle factors), and once we surpass that threshold, we begin to store exponentially more fat in our viscera, especially the liver and pancreas, which causes insulin resistance and metabolic dysfunction.3–6
If you want to actually cure type 2 diabetes, then you need to lose fat.
This has been unequivocally demonstrated by the Counterpoint and Counterbalance studies out of Newcastle University.7
In counterpoint,8 individuals with type 2 diabetes were placed on a meal-replacement diet providing about 600 kcal per day (60 g of carbs) for 8 weeks. They lost 15% of their body weight, reduced their liver fat content from 13% to 3%, and reduced their pancreatic fat content from 8% to 6%.
This extensive fat loss occurred alongside notable reductions in HbA1c, fasting glucose, fasting insulin, fasting triglycerides, as well as normalization of hepatic insulin sensitivity, the pancreatic response to glucose, and peripheral insulin sensitivity.


The Counterbalance Study built on these findings.9 The same intervention was used for 8-weeks, which was then followed by 6 months of eating normally and maintaining any weight loss.
Not only did glycemic control and insulin sensitivity improve as a result of substantial fat loss, but these improvement were maintained even when the participants started eating (gasp!) a normal amount of carbohydrate!
When the participants looked at the participants who responded well to treatment and those who did not, the non-responders simply didn’t achieve the same level of pancreatic fat reduction. In particular, nonresponders were characterized by evidence of insulin deficiency at baseline and lack of ability to regenerate insulin secretion capacity.
So, diabetes is completely curable in some individuals who do not have a level of pancreatic damage. And when I say cure, I literally mean that you can eat carbohydrates again without issue.
I’m all for a ketogenic diet to manage the symptoms of diabetes (elevated blood glucose and insulin levels), but it needs to be coupled with fat loss to address the diabetes itself.
Summing up
Diabetes is a condition often caused when someone surpasses their personal fat threshold. This causes an accumulation of fat in the liver and pancreas, causing metabolic dysfunction. The cure is simple: lose fat.
References
- 1.Athinarayanan SJ, Adams RN, Hallberg SJ, et al. Long-Term Effects of a Novel Continuous Remote Care Intervention Including Nutritional Ketosis for the Management of Type 2 Diabetes: A 2-Year Non-randomized Clinical Trial. Front Endocrinol. June 2019. doi:10.3389/fendo.2019.00348
- 2.Taylor R, Holman R. Normal weight individuals who develop type 2 diabetes: the personal fat threshold. Clin Sci (Lond). 2015;128(7):405-410. https://www.ncbi.nlm.nih.gov/pubmed/25515001.
- 3.Lafontan M. Adipose tissue and adipocyte dysregulation. Diabetes Metab. 2014;40(1):16-28. https://www.ncbi.nlm.nih.gov/pubmed/24139247.
- 4.Frayn K. Adipose tissue as a buffer for daily lipid flux. Diabetologia. 2002;45(9):1201-1210. https://www.ncbi.nlm.nih.gov/pubmed/12242452.
- 5.Haczeyni F, Bell-Anderson K, Farrell G. Causes and mechanisms of adipocyte enlargement and adipose expansion. Obes Rev. 2018;19(3):406-420. https://www.ncbi.nlm.nih.gov/pubmed/29243339.
- 6.Kim J, Huh J, Sohn J, et al. Lipid-overloaded enlarged adipocytes provoke insulin resistance independent of inflammation. Mol Cell Biol. 2015;35(10):1686-1699. https://www.ncbi.nlm.nih.gov/pubmed/25733684.
- 7.Taylor R, Barnes A. Translating aetiological insight into sustainable management of type 2 diabetes. Diabetologia. 2018;61(2):273-283. https://www.ncbi.nlm.nih.gov/pubmed/29143063.
- 8.Taylor R. Calorie restriction and reversal of type 2 diabetes. Expert Rev Endocrinol Metab. 2016;11(6):521-528. https://www.ncbi.nlm.nih.gov/pubmed/30058916.
- 9.Steven S, Hollingsworth K, Al-Mrabeh A, et al. Very Low-Calorie Diet and 6 Months of Weight Stability in Type 2 Diabetes: Pathophysiological Changes in Responders and Nonresponders. Diabetes Care. 2016;39(5):808-815. https://www.ncbi.nlm.nih.gov/pubmed/27002059.